Beyond Root, STJ Neutral & Pronation
|
The Rootian Theory of Lower Extremity Biomechanics, based upon STJ Neutral Diagnosis and Casting, is being questioned in the literature and peer podiatry practice by Payne, Levitz and others for being in need of upgrading and/or change.
STJ Neutral position is not accurate or reproducible and it is not the optimal casting position to use for fabrication of foot orthotics for most feet. Although it produces orthotics that reduce pain (so did arch supports), experts agree that STJ Neutral position can serve as a reference point for examination and diagnosis, but falls short when used for casting of orthotics and treatment of mechanical pathology. Speciously, these same investigators, for the most part, still use STJ Neutral casting resisting any change that does not agree with their own and the podiatry community seems hesitant to take a new fork in the biomechanical road.
Root, without proof, stretched the fact that the frontal plane is the only plane that can be measured with accuracy when monitoring STJ pronation into his theory that controlling STJ pronation on the frontal plane is the foundation for treating the foot biomechanically.
In Root, control of the frontal plane component (inversion-eversion) of tri planal subtalar pronation is the focus of biomechanical attention. Modern Biomechanists including Dananberg, Ritchie, Glaser and this author offer sagital plane correction, forefoot modifications and increased vaulting as potential upgrades overlooked or dismissed by those mandating rearfoot control (STJ Axis, Blake Inversion Casting.
Neoteric Biomechanics asks the question "If I don’t take a STJ Neutral cast and prescribe a three degree rearfoot post to treat most feet mechanically, what alternatives offer better diagnostic and treatment options?"
Since some feet are rearfoot weak, others are stable and many (remove still others) strong and since many forefoot are weak, others stable and some strong, a method of profiling all feet architecturally and classifying them into foot types according to their rearfoot and forefoot characteristics may be a valuable starting point for a new paradigm.
 |
It could explain the inherited nature of many foot deformities and performance issues. It would help predict when DPM’s should incorporate a forefoot post, additional Vault support, a heel lift or a first ray cutout instead of a varus rearfoot post for a given patient. It would help educate the foot suffering public and the medical community of the value of biomechanical compensation starting early in life by simplifying our language and it would eliminate most of the untrained and self-certified orthotic dispensing competitors from imitating the podiatry community denying them a place at the top of the biomechanical pyramid next to us that they currently enjoy.
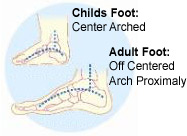
At birth, the bones forming the vault foot conform to an architectural vault in an engineering sense. They form a rearfoot and forefoot of equal length with a centrally placed keystone. This allows for great closed chain support but poor function. Miraculously, during the growth years, each bone stops growing at different stages of development, until at skeletal maturity, the architecture of the foot morphs into a vault that has a short rearfoot, a long forefoot and a proximally set keystone allowing our muscle engines to gain mechanical advantage in order to improve closed chain function. Measuring length, width and navicular sag over time determines the extent and location of this natural collapse within the foot that differs for each of us, foot type-specific. The fact that the rearfoot stops its growth first as the vault of the foot collapses and the forefoot lengthens and widens exposes the weaknesses in a paradigm like Roots that diagnoses and treats the rearfoot as the foundation of biomechanical pathology when the real fix lies elsewhere.
Although some feet pathologically collapse at an early age (congenital flat feet, juvenile bunions), for most of us, the cementing ligaments and muscle engines that power our feet weaken and stretch losing potential mechanical advantage in all of us, on a case to case basis, as we mature. These functional pulleys and levers become weak, underdeveloped and incapable of exerting sufficient control over a progressively more flexible, lengthened, widened and collapsed foot architecture. Because STJ Neutral casted orthotics capture these already collapsed and weakened feet, they fail to delay or reverse pathologic foot collapse and they cannot enable muscle engines to be trained because they have little effect on the vault and the forefoot.
I predict that the new and fresh road podiatry will take biomechanically in the future will be to foot type patients architecturally and then instead of STJ Neutral casting, we will learn to custom cast feet simulating the position that they were in when bone growth ended. This will prevent and/or reverse some pathological “Adult Expansion” and allow ligaments and muscle engines to strengthen and be trainable, according to Wolfs and Davis’ Laws with a renewed ability to support and power that Dr. Root only dreamed of. Podiatry orthotics will become shorter, narrower, higher arched and fully forefoot posted and foot type-specific and DPM’s who are skilled and passionate in practicing lower extremity biomechanics will lead the way.
The next installment: Diagnosing the Functional Rear Types
References:
Root, M.L., Orien, W.P., Weed, J.H., & Hughes, R.J. (1971). Biomechanical examination of the foot.
(Vol.1). Los Angeles: Clinical Biomechanics.
Root ML, Orien WP, & Weed JH. Normal & abnormal function of the foot. (19770 Clinical
Biomechanics Corporation, Los Angeles: Clinical Biomechanics
Morrison SC, Durward BR, Watt GF. Prediction of Anthropometric Foot Characteristics in Children, JAPMA, Volume 99 Number 6 497-502 2009
Chen Y, Yu G, Mei J, Zhou J. Assessment of subtalar joint neutral position: a cadaveric study.
Chinese Medical Journal, 2008, Vol.121 No. 8
Sobel E, Levitz, SJ. Reappraisal of the negative cast impression cast and subtalar neutral position.
JAPMA:1997;87(1):30-34
Elviru RA, Rothstein JM et al. Methods for taking subtalar joint measurements. A clinical report.
Phys Ther1998; 68(5):678-673
Payne, CB, Bird AR. Teaching clinical biomechanics in the context of uncertainty.
JAPMA, 1999 Vol 89, Issue 10 525-530
P.Cavanagh, E.Morag. The relationship of static foot structure to dynamic foot function
Journal of Biomechanics, 1997 Volume 30, Issue 3, Pages 243-250 |
|